Glomus Tumour (Paraganglioma of Temporal Bone)
Introduction
Glomus tumours, also known as paragangliomas or chemodectomas, are the most common benign tumours of the middle ear and the second most common tumours of the temporal bone. Glomus tumours was first described by Guild (Glasscock, 1982). Glomus tumour (paraganglioma of temporal bone) is a highly vascular, benign but locally aggressive tumour of the middle ear and skull base. It is the most common middle ear tumour and the second most common temporal bone tumour. It typically presents with pulsatile tinnitus, conductive hearing loss, and a red vascular middle ear mass. Despite being histologically benign, it can cause significant bone erosion and lower cranial nerve palsies. This topic is extremely important for NEET PG, INI-CET, FMGE, and ENT viva exams due to its characteristic imaging (salt & pepper appearance) and surgical classification (Fisch system).
Why is it Clinically Important? (CBME Must-Know)
- High Vascularity: Glomus tumours are notoriously vascular, leading to the characteristic symptom of pulsatile tinnitus and posing a high risk of profuse bleeding during biopsy or surgery.
- Local Aggression: Despite being histologically benign, they aggressively erode the surrounding bone, particularly the jugular foramen (Glomus Jugulare), causing multiple cranial nerve palsies (IX-XII).
- Clinical Mimicry: Their presentation can easily mimic common ear conditions like Chronic Suppurative Otitis Media (CSOM) with aural polyp, making accurate diagnosis essential.
Aetiology & Pathophysiology
1. Origin: Arise from neural crest-derived paraganglionic cells (glomus bodies), which are chemoreceptors.
2. Common Locations in the Temporal Bone:
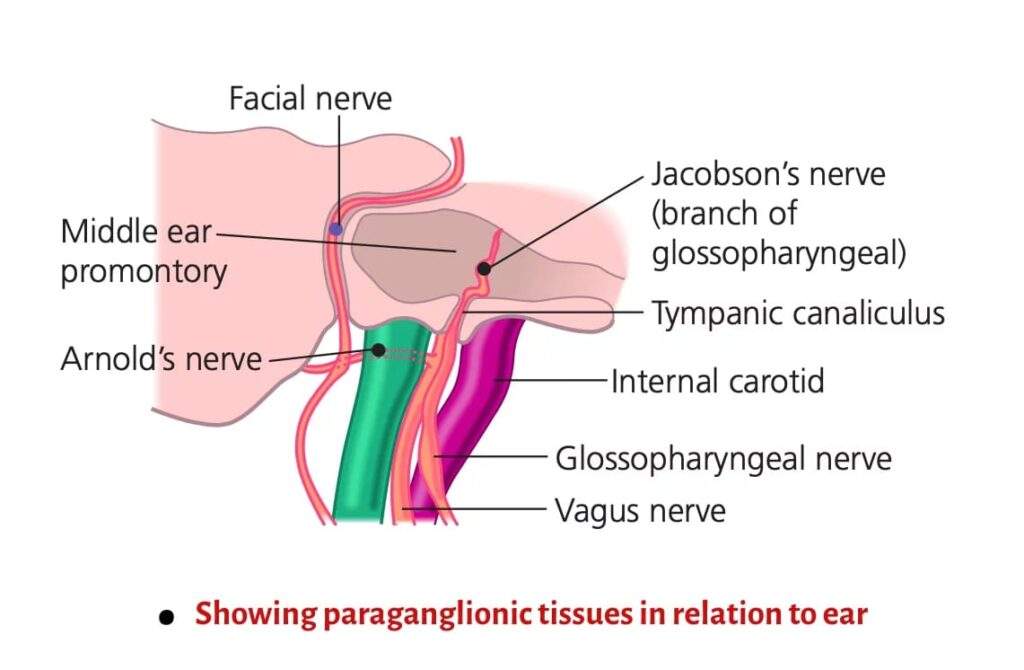
- Glomus Tympanicum: Arises from paraganglia on the promontory along the tympanic branch of the glossopharyngeal nerve (Jacobson’s nerve).
- Glomus Jugulare: Arises from paraganglia in the jugular bulb region, the ganglion of the vagus nerve (X), or along the auricular branch of the vagus nerve (Arnold’s nerve).
3. Nature: Slow-growing, nonencapsulated, but extremely vascular; metastasis is rare.
4. Feeding vessel (High-Yield Exam Question): The primary feeding vessel is the Ascending Pharyngeal Artery, a branch of the External Carotid Artery.
5. Demographics: Most often seen in the 5th and 6th decades of life, with a strong female predominance (5:1).
6. Familial occurrence: 10% familial, 10% multicentric (occurring in more than one site), and 10% functional (secreting catecholamines).
Pathology
Microscopically, the tumour exhibits masses or sheets of epithelial-like cells (Chief cells) arranged in a characteristic “Zellballen” pattern (nests of cells) separated by a delicate fibrovascular stroma. There is an abundance of thin-walled blood sinusoids with no contractile muscle coat, accounting for profuse bleeding from the tumours.
Macroscopically, all paragangliomas are firm, well-circumscribed lesions that are yellow, tan, brown or reddish in colour. They can have a thin, but focally thickened, fibrous capsule.
Common Sites of Paragangliomas
| Site | Type |
|---|---|
| Middle ear | Glomus tympanicum |
| Jugular fossa | Glomus jugulare |
| Carotid bifurcation | Glomus caroticum |
| Vagus nerve ganglion | Glomus vagale |
1. Glomus Tympanicum.
It is the most common middle ear tumour. It arises from the paraganglion located in the promontory. They are located along the tympanic branch (Jacobson’s nerve) of the glossopharyngeal nerve and the auricular branch (Arnold’s nerve) of the vagus nerve. In contrast to glomus jugulare, bone erosion is rare in glomus tympanicum (the hypotympanic floor, jugular fossa and ossicles are usually intact). A large tumour may cause a bulge of the tympanic membrane and a smooth indentation of the promontory, causing aural symptoms. Posteriorly, it may extend into the mastoid and inferiorly into the hypotympanic air cells and jugular fossa.
CT is the investigation of choice for diagnosis. Axial and coronal sections show a well-defined nodular area of soft tissue on the cochlear promontory. MRI is only indicated for larger lesions extending outside the middle ear cavity. It seldom requires preoperative embolisation and can be resected with conventional tympanoplasty techniques.

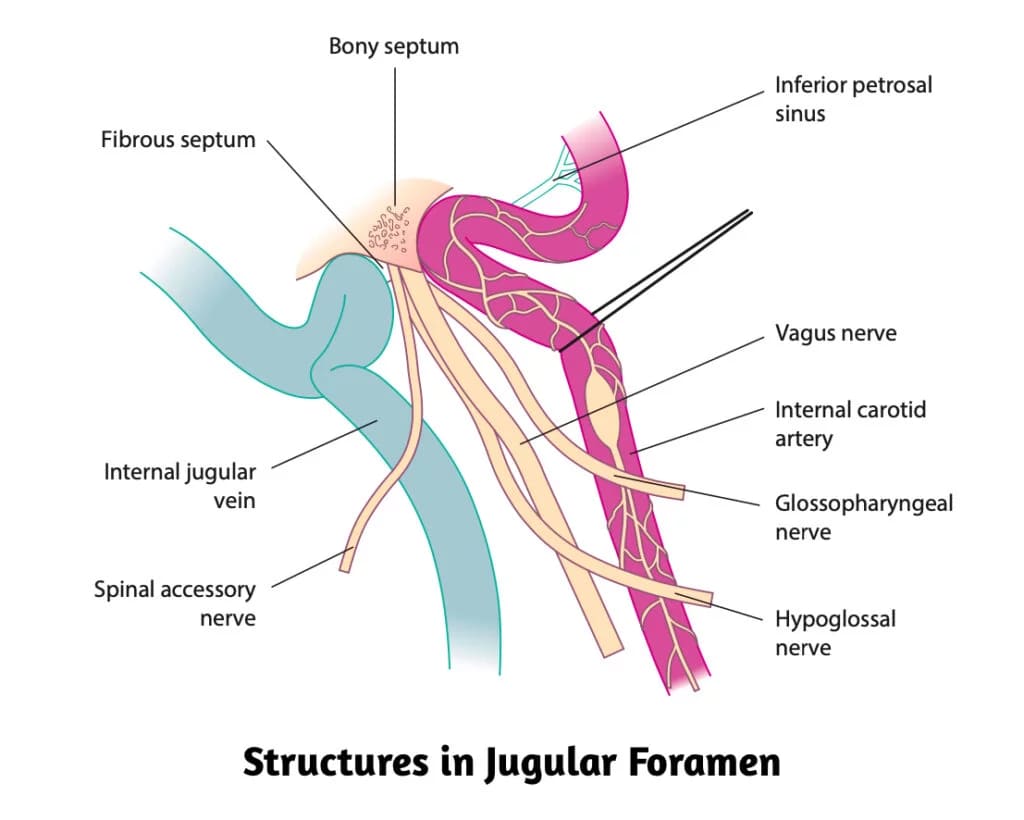
2. Glomus Jugulare.
It arises from the paraganglion located in the jugular bulb, the Xth nerve ganglion, and/ or from the Arnold or Jacobson nerves.
Glomus jugulare tumours erode the jugular fossa and break through the bony roof of the jugular fossa, causing neurological signs of IXth to XIIth cranial nerve involvement. Destruction of bone around the caroticojugular spine, jugular tubercle, and hypoglossal canal may also be seen. As the tumour increases in size, it causes erosion of the floor of the hypotympanum and may fill the entire middle ear cavity and from there into the external auditory canal.
Lateral extension of the lesion into the mastoid often leads to erosion of the facial canal and involvement of the facial nerve. Medially, it invades the petrous pyramid and destroys the perilabyrinthine bone and the petrous apex. Extracranially, it may compress the jugular vein or invade its lumen. Intracranial involvement is often observed in large tumours, although the lesion usually remains extradural.
Spread of Glomus Jugulare Tumour
- As the floor of the hypotympanum is eroded, the tumour extends superiorly into the middle ear cavity and later perforates through the tympanic membrane to present into the external auditory canal as a vascular polyp.
- It may invade the labyrinth, the petrous pyramid and the mastoid.
- It may invade the jugular foramen and the base of skull, causing IXth to XIIth cranial nerve palsies.
- By spreading through the eustachian tube, it may present in the nasopharynx.
- Intracranially, it may spread to the posterior and middle cranial fossae. Intracranial involvement is often observed in large tumours, although the lesion usually remains extradural.
- Metastatic spread to lungs and bones is rare, but is seen in 4% of cases. Metastatic lymph node enlargement can also occur.
Fisch classification for glomus tumours
It is the most widely used system for Glomus Tumours, as it is crucial for surgical planning and reporting outcomes.
| Fisch Classification Type | Extent of Tumour |
|---|---|
| Type A | Limited to the middle ear cleft. (Glomus Tympanicum) |
| Type B | Limited to the tympanomastoid area. (Glomus Tympano-Mastoid) |
| Type C | Involving the infra-labyrinthine compartment and extending into the petrous apex. (Glomus Jugulare) |
| C1 | Limited involvement of the vertical portion of the carotid canal. |
| C2 | Invading the vertical portion of the carotid canal. |
| C3 | Invasion of the horizontal portion of the carotid canal. |
| Type D | With intracranial extension. |
| D1 | Intracranial extension < 2 cm in diameter. |
| D2 | Intracranial extension > 2 cm in diameter. |
Clinical features
Almost 90% of skull base paragangliomas have conductive hearing loss and symptoms pertaining to the ear.
1. Pulsatile tinnitus and/ or hearing loss. The earliest symptoms are pulsatile tinnitus and/ or hearing loss. Tinnitus is swishing in character, synchronous with pulse and can be temporarily stopped by carotid pressure. A glomus tympanicum may present early with conductive hearing loss, which is slowly progressive in nature; whereas glomus jugulare may present with a mixed deafness when the middle and inner ears are both involved. There may be otalgia, ear fullness, otorrhea and aural bleeding.
2. Polypoidal mass. In advanced disease, the tumour may perforate the tympanic membrane and present as a red, vascular polyp in the external auditory canal that bleeds readily and profusely on touch.
3. Cranial Nerve Palsies. Involvement of the lower cranial nerves is a late, but definitive, sign of Glomus Jugulare:
- IX, X, XI, XII: Involved in the Jugular Foramen and lead to features like dysphagia, hoarseness, and tongue weakness. There is dysphagia and hoarseness with asymmetric palatal elevation or an abnormal gag reflex (IX, X) and dysarthria and hoarseness of voice due to unilateral paralysis of vocal cords (X) with weakness of the trapezius and sternomastoid muscles (XI) and deviation on protrusion, wasting and atrophy of the tongue (XII) nerves. Horner’s syndrome (ptosis, meiosis, anhydrosis and enopthalmus) can be observed.
- VII and VIII: Involved as the tumour spreads laterally into the mastoid and petrous bone. The facial nerve (CN VII) can be affected in advanced cases of glomus tympanicum.
- Order of Frequency of Involvement: VII > X > XII > IX > XI.
4. Dizziness, Earache (generally not present but differentiates it from carcinoma of the external and middle ear), Ear discharge (due to secondary infection), Tumour mass (over the mastoid or in the nasopharynx), Catecholamine symptoms (Headache, sweating, palpitation, hypertension and anxiety).
Signs (Physical Examination)
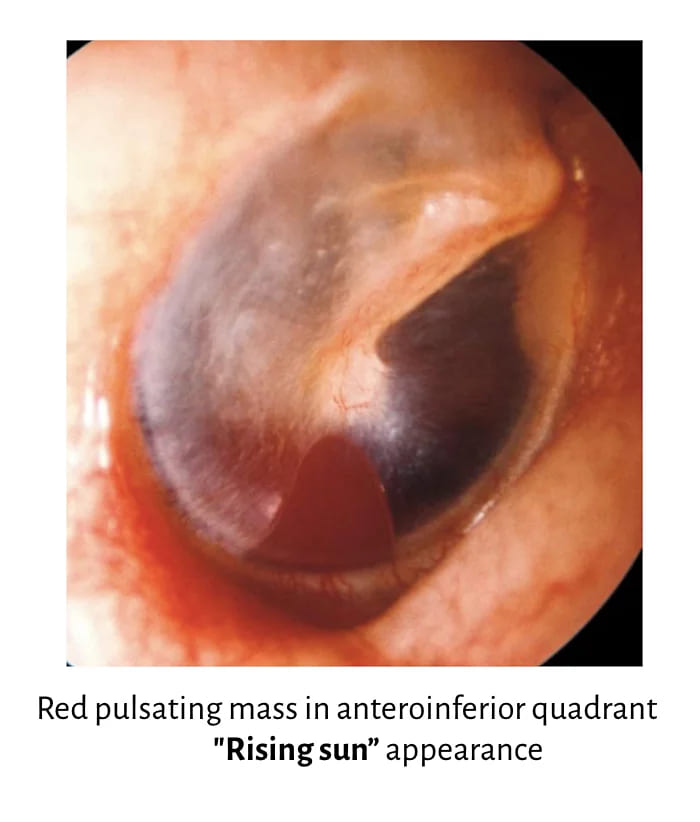
- Otoscopy. Reddish-blue reflex may be seen through an intact tympanic membrane. If the tumour is arising from the promontory, a red pulsatile mass may be seen behind the tympanic membrane, and a glomus tympanicum tumour is the most likely diagnosis. If the tumour is arising from the floor of the middle ear, ‘Rising sun appearance’ is seen, and glomus jugulare tumour is the most likely diagnosis. Tympanic membrane also appears blue in cases of haemotympanum (temporal bone fracture), glue ear, glomus tumour and haemangioma of the middle ear.
- Pulsation Sign (Brown’s Sign). When pressure in the ear canal is raised (e.g., with Siegel’s speculum), the tumour first blanches (becomes pale) and then pulsates vigorously (becomes red) upon release of pressure; the reverse happens with the release of pressure. Highly characteristic of a vascular middle ear mass (Glomus tumour).
- Auscultation. A systolic bruit can be heard over the mastoid or upper neck with a stethoscope. Confirms high vascularity and is indicative of underlying pathology.
- Lower Cranial Nerve Palsies. Palatal paresis (IX, X), vocal cord paralysis (X), sternocleidomastoid/trapezius weakness (XI), tongue atrophy/deviation (XII). A hallmark of Glomus Jugulare due to erosion of the Jugular Foramen.
- Biopsy of a suspected vascular middle ear mass is strictly contraindicated due to the risk of catastrophic haemorrhage.
- Inspection and palpation of the neck (cervical mass and trapezius weakness in extensive jugulotympanic glomus). Examination of the neck is also important in patients with glomus tumours to identify synchronous paragangliomas or detect direct extension of a large tumour into the neck (e.g. glomus jugulare or vagale).
- Inspection of the oral cavity and pharyngolarynx (tongue deviation, decreased gag reflex, vocal cord paresis in extensive jugulotympanic glomus).
Diagnosis & Investigations
A combination of CT, MRI, and Angiography is necessary for complete assessment.
1. Imaging Modalities (CBME/NEET PG Focus)
- CT Scan Head (Temporal Bone). It shows how much bone the tumour has eroded. In glomus tympanicum, it appears as a well-defined soft-tissue mass on the cochlear promontory with minimal bone involvement. In contrast, glomus jugulare shows erosion of the caroticojugular spine, and erosion of this spine helps distinguish it from glomus tympanicum. CT scan is also useful for differentiating these tumours from other conditions, such as an aberrant internal carotid artery or a high-riding or dehiscent jugular bulb.
- MRI. It is the best investigation to assess the soft-tissue extent of the tumour, including its size, intracranial or extracranial spread, and involvement of nearby vessels. A classic high-yield feature on T1-weighted MRI is the “salt and pepper” appearance, where the “pepper” represents flow voids from fast-moving blood in tumour vessels, and the “salt” comes from tiny areas of haemorrhage. MRI clearly shows how far the soft tissue component has spread, while MR angiography and venography help identify invasion of the jugular bulb or vein and detect any compression of the carotid artery.
2. Four-Vessel Angiography. Vascular mapping and embolisation are important for planning surgery in glomus tumours. They identify the main feeding vessel—usually the ascending pharyngeal artery—and detect any additional lesions. This is especially needed when CT shows involvement of the jugular bulb, carotid artery, or intradural extension. Mapping also helps locate all feeding vessels and allows preoperative embolisation to reduce surgical bleeding.
3. Biochemical Tests (Catecholamine Secretion): needed when a glomus tumour is suspected to be functional and producing catecholamines. In such cases, 24-hour urinary metanephrines and vanillylmandelic acid (VMA) are measured to confirm or rule out hormone secretion. Serum catecholamine levels or their breakdown products can also be assessed when required.
4. Brain Perfusion and Flow Studies. They are necessary when the tumour is pressing on the internal carotid artery. If the case needs surgery, brain perfusion and adequacy of the contralateral internal carotid artery and the circle of Willis can be assessed. If needed, xenon blood flow and isotope studies are done for precise blood flow, and the risk of stroke and need for surgical replacement of the internal carotid artery.
5. Pure tone and speech audiometry to assess the type and degree of hearing loss. Vestibular function tests for dizziness or vertigo.
Treatment
The management depends on the tumour size, location, patient’s age, and symptoms.
1. Surgery: This is the primary treatment for most patients. Approach depends on Fisch Type:
- Type A: Transcanal tympanotomy.
- Type B/C: Mastoidectomy + Facial Recess Approach.
- Large Type C/D: Infratemporal Fossa Approach (Fisch Approach) – which requires anterior transposition of the facial nerve.
2. Radiation Therapy (RT): RT (including Stereotactic Radiosurgery) may be appropriate for tumours impossible to remove surgically, having intracranial extension, residual tumours, or for old patients with limited life expectancy. The aim is to reduce its vascularity and bring about sclerosis and fibrosis, hence arrest its growth. It is an excellent option for:
- Inoperable tumours.
- Elderly or high-risk surgical patients.
- Residual or recurrent disease.
- Tumours with significant intracranial extension.
3. Pre-operative Embolisation: This is a standard of care for larger tumours (especially glomus jugulare). Therefore, it is performed 24-48 hours before surgery to reduce vascularity, thereby minimising blood loss and providing a clearer surgical field. Embolisation can also be done in inoperable patients who have received radiation. Gelfoam and coils can be used in feeding vessel occlusion proximal to the tumour. Gelfoam powder is derived from pork-skin gelatin.
4. Combination of the above techniques.
Differential Diagnosis
It is important to differentiate Glomus Tumours from other reddish-blue masses behind the intact TM (NEET PG High-Yield):
- Glomus Tumour
- High/Dehiscent Jugular Bulb (appears dark blue/purple)
- Aberrant Internal Carotid Artery (seen in the anterior mesotympanum, does not have a positive Brown’s Sign)
- Haemotympanum (blood behind the TM, usually post-trauma)
- Haemangioma of the middle ear
———— End of the chapter ————
High-Yield Points for NEET PG & University Exams
- Glomus tympanicum is the most common middle ear tumour; glomus jugulare is the second most common temporal bone tumour after vestibular schwannoma.
- Glomus tympanicum arises from Jacobson’s nerve (tympanic branch of glossopharyngeal nerve, CN IX) on the cochlear promontory.
- Glomus jugulare arises from Arnold’s nerve (auricular branch of vagus nerve, CN X) in the jugular bulb region.
- Primary feeding vessel is the ascending pharyngeal artery (branch of external carotid artery) – frequently tested in NEET PG.
- Fisch Classification: Type A (promontory), Type B (mastoid), Type C (infralabyrinthine/petrous apex), Type D (intracranial) – memorize this sequence.
- Surgical approach for Type A: Transcanal tympanotomy; Type B/C: Mastoidectomy + facial recess approach; Type D: Infratemporal fossa approach (requires facial nerve transposition).
- Classic microscopic pattern: Zellballen (nests of chief cells surrounded by fibrovascular stroma) – pathognomonic for paraganglioma.
- Classic MRI finding: “Salt and pepper” appearance on T1-weighted imaging – pepper = flow voids (vascular channels), salt = haemorrhage foci.
- Brown’s sign: Mass blanches with positive pressure (Siegel’s speculum) and pulsates vigorously on release – pathognomonic of vascular middle ear mass.
- Order of cranial nerve involvement (most to least): VII > X > XII > IX > XI – high-yield viva question.
- 10-10-10 Rule of Glomus Tumours: 10% familial, 10% multicentric, 10% functional (catecholamine-secreting).
- Female predominance: 5:1 female-to-male ratio; peak incidence in 5th-6th decades.
- Absolute contraindication: Biopsy – risk of catastrophic haemorrhage from the highly vascular tumour.
- Preoperative embolisation: Performed 24-48 hours before surgery using gelfoam or coils – standard of care for glomus jugulare.
- Metastasis rate: Approximately 4% (lungs and bones) – despite being histologically benign.
- Most common symptom: Pulsatile tinnitus (swishing, synchronous with pulse, stops with carotid pressure).
- Most common hearing loss type: Conductive (glomus tympanicum); mixed (glomus jugulare with inner ear involvement).
- Rising sun appearance: Red mass arising from the floor of the middle ear – indicates glomus jugulare (otoscopy sign).
- Intracranial extension: Usually remains extradural – important surgical planning point.
- Functional tumour management: Preoperative alpha-blockade (phenoxybenzamine) followed by beta-blockers only after adequate alpha-blockade.
NEET PG-Style MCQs
- The most common middle ear tumour is: A. Vestibular schwannoma B. Glomus tympanicum C. Glomus jugulare D. Meningioma.
- The primary feeding vessel of glomus tumours is: A. Internal carotid artery B. Ascending pharyngeal artery C. Maxillary artery D. Posterior auricular artery.
- The characteristic microscopic appearance of glomus tumours is: A. Verocay bodies B. Zellballen pattern C. Psammoma bodies D. Keratin pearls.
- The “salt and pepper” appearance on MRI is characteristic of: A. Vestibular schwannoma B. Meningioma C. Glomus tumour D. Cholesteatoma.
- Brown’s sign is positive in: A. Cholesteatoma B. Glomus tumour C. Otosclerosis D. Meniere’s disease.
- The Fisch classification for glomus tumours includes all EXCEPT: A. Type A (promontory) B. Type B (mastoid) C. Type C (infralabyrinthine) D. Type E (epidural).
- The most common cranial nerve involved in glomus jugulare is: A. IX (Glossopharyngeal) B. X (Vagus) C. VII (Facial) D. XII (Hypoglossal).
- Biopsy of a suspected glomus tumour is contraindicated because of: A. Risk of infection B. Risk of catastrophic haemorrhage C. Risk of tumour seeding D. Risk of facial nerve injury.
- Glomus tympanicum arises from: A. Arnold’s nerve B. Jacobson’s nerve C. Jugular bulb D. Carotid body.
- Preoperative embolisation for glomus tumours is typically performed: A. 1-2 hours before surgery B. 24-48 hours before surgery C. 1 week before surgery D. 2 weeks before surgery.
MCQs Answers: 1: B. 2: B. 3: B. 4: C. 5: B. 6: D. 7: C. 8: B. 9: B. 10: B.
Clinical Case Scenarios for Practical Exams & Viva
1. Case 1. A 55-year-old female presents with right-sided pulsatile tinnitus and progressive hearing loss for 6 months. Otoscopy reveals a reddish-blue reflex through an intact tympanic membrane. On applying pressure with a Siegel’s speculum, the mass blanches and then pulsates vigorously. Pure tone audiometry shows conductive hearing loss. Most likely diagnosis: Glomus tympanicum (Fisch Type A). Best investigation: CT scan temporal bone showing soft tissue mass on promontory with minimal bone erosion. Best management: Surgical resection via transcanal tympanotomy.
2. Case 2. A 60-year-old female with hypertension presents with hoarseness, dysphagia, and right-sided hearing loss for 1 year. On examination, she has right vocal cord palsy, palatal paresis, and tongue deviation to the right. Otoscopy reveals a red pulsatile mass behind the tympanic membrane. MRI shows a “salt and pepper” lesion in the jugular foramen with intracranial extension. Most likely diagnosis: Glomus jugulare with lower cranial nerve palsies (Fisch Type D). Best investigation: Four-vessel angiography to identify feeding vessels and assess carotid involvement. Best management: Preoperative embolisation followed by surgical resection via infratemporal fossa approach.
3. Case 3. A 45-year-old female presents with palpitations, headache, sweating, and a red mass behind the right tympanic membrane. She has a history of similar symptoms during previous minor procedures. Most likely diagnosis: Functional glomus tumour secreting catecholamines. Best investigation: 24-hour urinary metanephrines and VMA. Best management: Preoperative alpha-blockade with phenoxybenzamine, then surgical resection.
4. Case 4. A 70-year-old male with multiple comorbidities and a 3 cm glomus jugulare tumour refuses surgery. He has progressive hearing loss but no cranial nerve palsies. Most likely diagnosis: Glomus jugulare in an elderly patient. Best management: Stereotactic radiosurgery (Gamma Knife) to arrest tumour growth and preserve neurological function.
Frequently Asked Questions in Viva
- Q: What is the difference between glomus tympanicum and glomus jugulare? A: Glomus tympanicum arises from Jacobson’s nerve on the promontory and is confined to the middle ear, causing conductive hearing loss and pulsatile tinnitus. Glomus jugulare arises from the jugular bulb and causes lower cranial nerve palsies (IX-XII) in addition to ear symptoms.
- Q: Why is biopsy contraindicated in glomus tumours? A: Biopsy is strictly contraindicated because glomus tumours are extremely vascular. Biopsy carries a high risk of catastrophic haemorrhage, which can be life-threatening. Diagnosis should be based on imaging (CT and MRI).
- Q: What is Brown’s sign? A: Brown’s sign is a pulsation sign observed during otoscopy. When pressure is applied with a Siegel’s speculum, the glomus tumour blanches (becomes pale) and then pulsates vigorously upon release of pressure. This sign is pathognomonic for vascular middle ear masses.
- Q: What is the classic MRI finding in glomus tumours? A: The “salt and pepper” appearance on T1-weighted MRI is characteristic. The “pepper” represents flow voids from fast-moving blood in tumour vessels, while the “salt” comes from tiny areas of haemorrhage within the tumour.
- Q: What is the Fisch classification? A: The Fisch classification is the most widely used system for glomus tumours: Type A (confined to promontory), Type B (mastoid involvement), Type C (infralabyrinthine and petrous apex), and Type D (intracranial extension). It guides surgical approach and predicts outcomes.
- Q: What is the primary treatment for glomus tumours? A: Surgery is the primary treatment for most patients. The approach depends on the Fisch type: transcanal tympanotomy for Type A, mastoidectomy for Type B/C, and infratemporal fossa approach for Type D. Radiation therapy is used for inoperable tumours or elderly patients.
- Q: What are the red flag signs that suggest complications? A: Lower cranial nerve palsies (IX-XII) suggest jugular foramen involvement. Facial nerve palsy suggests lateral spread into the mastoid. Catecholamine symptoms (headache, sweating, palpitations) indicate a functional tumour. Any of these requires immediate investigation.
———— End of the chapter ————
Download full PDF Link:
Glomus Tumour Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Glomus tumour ear, Glomus jugulare tumour, Symptoms of glomus tumor in ear, Glomus tympanicum tumor treatment, ENT diagnosis of glomus tumor, Pulsatile tinnitus glomus tumor, Surgery for glomus tumor in ear, Causes of glomus tumor, MRI features of glomus tumor, Glomus tumor case study ENT, Glomus tumor vs acoustic neuromaglomus jugulare complications, Vascular tumor middle ear, Paraganglioma ear tumor, Ear tumor ENT notes, Glomus tumor PDF notes, Glomus tumor NCERT, Glomus tumor larynx ENT, Red mass behind tympanic membrane, Pulsation sign, Rising sun appearance, Glomus tympanicum, Glomus jugulare, Glomus caroticum, Glomus vagale, Glomus tumour, Paraganglioma, Glomus tumour diagnosis, Symptoms of glomus tumor, Glomus jugulare treatment, Paraganglioma vs glomus tumour, Imaging for glomus tumors, Glomus tumour surgery outcomes, Causes of glomus tumor, Glomus tympanicum diagnosis, Rare vascular tumours ear, Glomus tumour hearing loss, Skull base paraganglioma, Glomus tumour ENT approach, Genetic link glomus tumor, Recurrence glomus tumours, Glomus tumour notes, Glomus jugulare summary, Glomus tympanicum MBBS notes, Temporal bone paraganglioma revision, Glomus tumour symptoms for exams, Glomus tumour diagnosis CBME, Glomus tumour treatment ENT PG, Fisch classification notes, Paraganglioma ENT short notes, Glomus tumour MCQs NEET PG, ENT exam guide glomus tumour, Glomus tumour viva questions, Glomus tumour management summary, Skull base paraganglioma notes, Middle ear tumour exam-oriented notes, Glomus Tumour ENT Notes for MBBS & PG Exams, Glomus Jugulare Exam Guide for ENT Students, Glomus Tympanicum CBME Summary & MCQs, Paraganglioma of Temporal Bone Study Notes, High-Yield ENT Revision: Glomus Tumour
Well, that’s good 👍